![]()
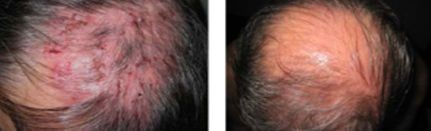
The most common form of the disorder and occurs when antibodies attack Desmoglein 3.
Sores often originate in the mouth, making eating difficult and uncomfortable.
Although pemphigus vulgaris may occur at any age, it is most common among people between the ages of 40 and 60.
It is the most common subtype of pemphigus, accounting for 70% of all pemphigus cases worldwide


![]()
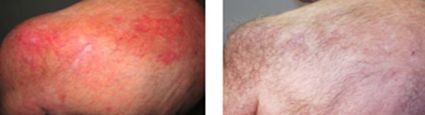
The least severe of the three varieties.
Desmoglein 1, the protein that is destroyed by the autoantibody, is found in only the top dry layer of the skin.
PF is characterized by crusty sores that often begin on the scalp, and may move to the chest, back, and face.
Mouth sores do not occur. It is not as painful as pemphigus vulgaris, and is often mis-diagnosed as dermatitis or eczema
Although pemphigus vulgaris may occur at any age, it is most common among people between the ages of 40 and 60.
It is the most common subtype of pemphigus, accounting for 70% of all pemphigus cases worldwide.


![]()
A group of newly characterized immune-mediated intraepidermal blistering skin diseases.
Unlike typical immunoglobulin G (IgG)–mediated pemphigus, IgA pemphigus is characterized by tissue-bound and circulating IgA autoantibodies that target the desmosomal proteins of the epidermis.